Though it is
almost four million years since the predecessor of Homo Sapiens first started walking on Terra Firma it is
barely 20 years since a new species Homo Computericus
evolved. For several millennia it was taken for granted that preventing,
diagnosing, treating diseases and maintaining health depended entirely on
Man’s innate physical skills. In the last decade it has been shown that
computers can be used in clinical practice in a way totally unthinkable
earlier. This article will attempt to do some crystal ball gazing and
take a look at where Homo Computericus is going
in the field of clinical practice. The basis of learning today is to know
where the information is available, and have a broad idea of the road
which one needs to take even if it is one less travelled by rather than
get bogged down by a myriad of inconsequential details. Therefore this
article will follow an unconventional method of purely attempting to
stimulate the reader without necessarily whetting the appetite!
Advantages of using computers in clinical situations:
More efficient data gathering
Provide immediate feedback to
patients
Overcomes problems of illegibility
Overcomes problems of inefficient
coding of data
Better data quality
Patient evaluation, compared to
written tests, may be less daunting than a long test list
Tireless, i.e. the same response
irrespective of the time of day
May be cost effective despite
Initial capital and costs in updates and maintenance
Health information management (HIM)
is concerned with health-related information and the management of
systems to collect, store, process, retrieve, analyse, disseminate and
communicate information related to the planning, provision, research and
evaluation of healthcare services
Hospital Information Systems
Laboratory automation - today almost
every single type of laboratory investigation is automated. Large numbers
can be done with precision in a cost effective manner.
Imaging – Ultrasound, Digital X
rays, 3D Spiral CT, 4 Tesla MRI. PET, SPECT etc
will eventually fuse into single multipurpose imaging with image fusion
software.
Intranets in large hospitals will be
commonplace.
Disadvantages
of using computers in clinical situations:
Initial capital outlay for hardware
and software
Costs in updates and maintenance
Administrative staff costs, Storage
and rooms
Staff training
Patients may decline to use
computers or may not have the requisite skills
Use of computers in a patient's home
may be impractical
Inhuman!
Best informed patients may
become "cyberchondriacs"
Prolonged clinical encounters due to
better informed patients
Information providers trying to
manipulate the general public to suit their own clinical or
administrative needs . Erroneous information
available on the net.
Intangible human skills eg intuition, experience, imagination cannot be
duplicated
Table 1
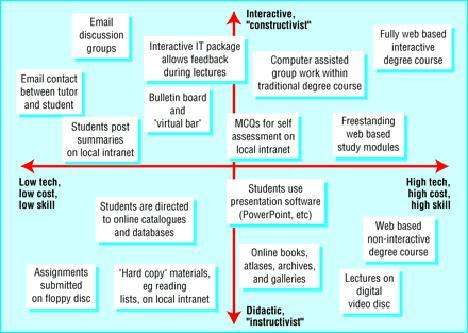
Computer Assisted Medical Education:
Table II Palmtops - Clinical Information -
Anytime, Anywhere
Looks up data on diagnosis of different diseases
and its treatment
Looks for drug interactions
Stores summaries of sick patients, including
their drugs lists
Reminds the doctor of necessity for uncommon
investigations Eg an ultrasound for evaluating
back ache (abdominal aortic aneurysm !)
Medical programs can be downloaded directly off
the Web.
Task schedules alerted with alarm.
Getting hard copies of important documents by
connecting to a printer.
Surf websites and send
& receive email – better than a WAP mobile phone.
Address book, schedules,Jotting down notes, tips, ideas.
During lectures and conferences notes can be
taken easily, and beamed using the infrared port to colleagues
absent in body, or in mind!!.
As much clinical information as required can be entered.
Blood results can be entered, and brought on
Ward Rounds.
Handovers can be printed
and discharge summaries produced.
Medikit I calculates medical and paediatric parameters,
from infusion rates to creatinine clearances, PEFRs to Anion gaps, Ransons Criteria to APACHE 2 scores. It will
even work out fluid rates and drug calculations for children
dependent on age.
British National Formulary Qcite
is a reference manager which organises Medline searches.
MaxSacs program, customisable for any specialty, allows
easy OPCS coding of operations, and enables rapid collection of data.
Medinotes is a large compendium of useful
information in many specialities.
Pre-programmed templates and drop-down menus for
entering history.
Generating electronic prescriptions. A growing
number of companies provide software for PDA-based prescriptions. The
doctor picks the drugs and the system knows if it's on the formulary; The
PDA then can be placed in its cradle or docking station, from which it
sends the prescription to a printer to be faxed to the pharmacy, or sends
it electronically to the pharmacist's fax number. Wireless devices that
enable real-time synchronization and transmission of information can also
be used.
Mobile technology can be used for home health
and emergency services. Only two minutes are required to Hot Sync a full
week's data into the practice management system.
A physician directory lookup, secure access to
confidential patient information, and wireless order processing for books
and articles from the medical library is all available on the palmtop.
Easy, ubiquitous access to online health care
data.
Proliferation of PDA’s in health care can help
break down barriers between clinicians and greater use of I.T. in
general.
As of October 2000, 15% of
physicians in the UK used handheld devices for reference purposes
such as scheduling and checking drug dosages 20% of physicians will be
using handheld devices for daily transactions by 2004, predicts a report
by WR Hambrecht + Co.
Hot-Sync – simple method of transfer
of data from and to computer,
Table III Limitations Of Palmtops in Clinical
Practice:
Danger of the device being lost or stolen
Dependence on the gadget
Incompatability between two different types of
palmtops
Infra red communication interfering with other
devices
Garbled information if multiple users in the same location use infra red portals
Colour
palm tops require periodic battery change
VIRTUAL REALITY IN CLINICAL PRACTICE:
Airline pilots spend weeks in
flight-simulators before even seeing a 747. They can also be
automatically assessed at the same time. Questions are being asked as to
why a trainee surgeon has to acquire skills on a real living patient –
exposing the latter to avoidable dangers. This has resulted in major
developments in VR for surgical training
The term "Virtual
Reality", is itself an oxymoron. Other terms that have been used are
Synthetic Environments, Cyberspace, Artificial Reality and Simulator
Technology. Virtual Reality (VR) is the most common and “sexiest”. It has
caught the attention of the media. Production of realistic 3D sensual
model from complex data. CT, MRI, fMRI,
MRA, US, Angio, PET, SPECT requires massive data manipulation using Workstations and
Minicomputers.
|
VR comprises a variety of
technological advances that allow computers to produce a realistic
dimensional and sensual model from complex data, with which humans can
then interact and manipulate. The individual is thus ‘immersed’, as if
‘teleported’ into the new world.
The visualisation part refers to the computer
generating visual, auditory or other sensory outputs to the user of a
world within the computer. This world may be a computer assisted design
model, a scientific simulation or a view into a database. The user can
interact with the world and directly manipulate objects within the
world. Some worlds are animated by physical simulations, Interaction and manipulation is possible in this
virtual world.
VR has particularly been used is in the field of laparascopic and arthroscopic surgery, where the
requisite skills required to perform the procedures entail a
steep
|

|
|
learning curve. Model knees that flex and
|
|
|
extend with a realistic skin cover are now available.
Acquisition of remote hand-eye coordination and indirect fine motor
control within a limited environment is the goal of VR simulation.
To produce the sensory outputs
required to generate an impression of reality, a number of different
Output Devices may be used.
|


|
|
|
VR interactive viewing of the brain
|
Uses of VR: Virtual Reality has the
distinct advantage of being able to turn an abstract situation into a
perceptibly real one .
For example a virtual world can be produced where the patient is immersed
in their phobic situation, and guided through therapy. VR can provide a
safe learning environment for development of skills needed to drive a
powered wheelchair.
VR may be utilised in surgery, for
planning and assisting. A virtual image is displayed upon the patient
over the operative site, A patient in a remote area can be examined by a
Physician using a haptic input / haptic output system. Simply put,
tactile information can be inputted at the source using
either a robotic hand or a volumetric sensor, and can be felt by the
examiner through a tactile output
Education, Training Simulation
Systems
Image Manipulation, Surgical
Guidance and Navigation Systems
Telepresence Surgery, Virtual
Telemedicine.
Robotics in clinical practice:
A robot is a reprogrammable, multifunctional manipulator designed to
move material, parts, tools, or specialized devices through various
programmed motions for the performance of a variety of tasks.
Improves accuracy or
reproducibility, or replaces lost physical abilities
Useful in Interventional Medicine
Useful in Open Surgery, Minimally Invasive
Surgery
Useful in Telepresence Surgery
Useful in Prosthetics ,Cybernetics
Useful in CAD-CAM Technology
Using complex 3D image reconstructions, robots can be used
to precisely target and deliver therapeutic agents to deep lesions such
as neoplasms. This allows pinpoint accuracy in delivery, provided that
the image reconstruction is perfect and the registration of patient data
to the robot is accurate.
A computer–robot can perform the
appropriate bone cuts required to seat a total knee replacement with
laser guided accuracy. With robot systems, it is possible to encode this
mirror imaging and use a robot to perform the manoeuvres, under operator
control. The operator uses a joystick or similar device to manipulate the
robot, with this important difference: the operator’s hand movements are
‘real sense’ or equivalent to the instrument movements, and so are intuitive
Robotic surgical systems do not need
to be controlled locally. Indeed, it may be more advantageous to be able
to control the robot from a distance, for example in remote areas or
where there is risk of infection. The main problem with such a system is
the bandwidth of the connection between the robot/sensing system and the
remote operator
An
individual with a Bionic prosthesis may be termed a Cybernetic Organism
or Cyborg for short. These are usually replacements for
musculoskeletal deficits and take the form of robotic arms or legs.
Increasingly sophisticated prostheses have been developed and applied.
Examples include powered lower leg prosthesis for amputees, which use
pneumatic technology to decrease the effort required whilst walking. The
physical interface between patient and prosthesis is paramount in
obtaining a good fit, thus restoring optimum function and preventing
pressure induced complications. If the patient’s limb stump is precisely
digitized into a three dimensional computer model, a computer driven
robot can then accurately fashion a matching socket, which will be
anatomically correct.
Medical
telemetry:
Measurement of physiological
parameters at a distance from the patient by cable, or by wireless
technology.
Biosensors are electrical components
which detect physiological parameters and convert them to digital values
e.g. a pulse oxy meter probe to detect the saturation of
capillary blood
ECG, temperature, oxygen saturation,
BP and respiration.
Fetal cardiography
Sleep apnoea alarms in Sudden Infant Death Syndrome
Dedicated radio-frequency spectrum
with sufficient bandwidth.
Artificial
intelligence in Clinical practice:
A System giving expert advice,
understanding “natural” computer languages, speaking like humans and
recognising complex patterns like handwriting is an AI system.
AI models for medical imaging,
cardiac, electrical, biomechanical behaviours, circulatory dynamics and
renal function are available.
Receiving and processing visual, auditory and tactile sensation
is a major function of intelligence. Intelligence, however cannot be
broken down to its constituent parts – the whole being greater than the
sum of its parts.
Useful AI Programs include expert systems, natural language
and neural networks.
An expert system can solve real world problems by following
the same IF/THEN rules a human expert follows. A software knowledge
engineer interviews one or several experts and encodes their thinking
process into the software knowledge base. The IF/THEN rules become expert
software knowledge frames. Expert systems are useful for simple medical
diagnosis and problem solving. Natural language software is the branch of
AI that focuses on enabling computers to understand spoken or typed
language. A neural network is a digitized model of a human brain,
simulated in the binary memory of a personal computer. A neural network
is made up of artificial neurons, connected to each other by weights
indicating the strength of the connection. As a neuron becomes energized
by input, it fires, sending a digital message to other neurons. There are
hundreds or even thousands of these inter-linked neurons, arranged in
layers, and all together they form a neural network, capable of learning
from experience.
Programs may be designed to serve as
consultants on complex problems where outstanding feats of pattern
recognition are required
AI may overcome human factors like data
overload, vigilance, varying expertise and human error.
Decision
support system:
·
Decision-making is a complex process based on the evaluation of available
data. Decision making ideally should be based on hard evidence which
takes into account every possible factor. In clinical practice this is
often based on “Intuitive reasoning” (an oxymoron?) based on one’s
“experience”. Consensus decision by a committee with different
types of experts treating the same disease in different ways may be
preferable to unilateral biased decisions. With state of the art neural
networks it should be possible to design an intelligent system which
could give correct unbiased weightage to different influencing factors
and arrive at a scientifically valid conclusion
·
How can a system ‘make decisions’? Can a decision be equated to
choosing between one of many alternatives. Does a Decision
Support System (DSS) merely sort things into ‘either-or’ categories? Can
a Neural Network mimic human ways of looking at data? Will the
Bayesian methods of calculating the probability of different outcomes
suffice? Is ‘Conditional Probability’ (A way of relating the
probability of an event to the presence of certain factors) evaluation
the answer? In clinical decision-making, there may be an information
overload with irrelevant facts. How does one separate the wood from the
trees? Can a DSS help one make better decisions? A DSS need not be
a rival but can be yet another aid with the physician still continuing to
call the shots.
·
Will it be possible to precisely identify specific characteristics, which
could predict suitability for a specific treatment? Which technique
should be used to identify these factors? Does the technique
matter? It is not always a matter of two different answers - the
techniques of the DSS and “clinical judgement” may be different
routes to the same answer. Categorizing data should yield more
information and this should make a difference
A Neural network which is the heart
(or rather the brain!) of a DSS should simulate the biological way of
connecting many artificial ‘neurons’ and training the network to
recognise patterns. The optimal arrangement of the ‘nodes’ (or neurons)
and training strategy are important. Neural Networks consist of a
series of linked ‘nodes’, linked to form a network. Nodes have layers
–input and output layers. Simple networks have no intervening layers.
Activation of each node occurs once its threshold is reached, and this is
determined by the summation of its inputs. Each input is also ‘weighted’,
so that some inputs are more important than others. A decision node can
be deleted if it doesn’t matter in practical terms which option is
taken. The danger of this approach is that we are determining before hand what information may be useful and what
may not be useful. It might then be difficult to include some new
item of information into the decision making process. One of the
strengths of Neural Networks, is integrating multiple pieces of
‘low-value’ information.
Conclusion: We
have come a long way since the Abacus was first thought of. To one trained
in the BC era (Before Computers) the future is sometimes frightening.
Many of us desperately cling to the present not realizing that we have
already become the past. The only thing that is constant in the
universe is change and we have to accept it, and the problem with the
future is that it is always ahead of schedule. At the same time we should
realize that “a fool with a tool is still a fool”. Technology in search
of an application is not the answer. Let us not become slaves of
technology but continue to be the master, never forgetting that no
supercomputer of the future can ever match the human brain whose circuits
will always remain a mystery. As the technology progresses we
can count on healthcare
software development companies to design, develop and deploy software
that matches the medical technologies of tomorrow.
We
have come a
|